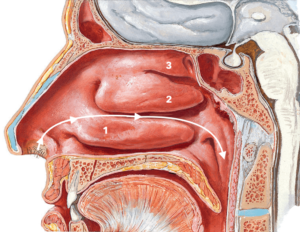
The three nasal turbinates are shelves on the internal lateral wall of the nose, which increase the functional surface of the nasal mucosa and help in the smooth flowing of the inspired air towards the throat and from there to the lungs. The inferior turbinate, which is the lowest of the three, serves as the regulator of the air flow. When the temperature of the environment is low, the head of the inferior turbinate swells up and the inflow of the air slows down, giving time to the nasal mucosa to warm the cold air. The opposite happens when the inhaled air is hot. Chronic Rhinitis often deregulates this mechanism, and with time causes permanent swelling of the turbinate, which contributes to the nasal obstruction. If this hypertrophy does not respond to topical medical treatment, surgical reduction of the turbinate can be offered.
There are a number of different methods, that can reduce the volume of the turbinates and increase the free space of the nostril. The modern tendency is not to apply aggressive methods, as the loss of mucosa and the alteration of the anatomy can impair the function of the nose. Nevertheless, there are cases, where surgery can indeed help. The main categories of surgical procedures to the turbinates are summarized below:
Turbinectomy: Surgical removal of the turbinate or part of it, is called Turbinectomy. It alters the anatomy and disturbs the normal paths of the air flow in the nose; often the patient feels that he/she cannot breathe, even when the nasal cavity is wide open (empty nose syndrome). Also, it is an aggressive operation, with a possibility of significant intraoperative or postoperative bleeding. This is why turbinectomy is not considered an acceptable option in our time, despite its extensive application in the past.
Cautery: Electrocautery, Laser or Radiofrequency (microwave) cautery produces a controlled burn in the mucosa of the turbinate. The resulting scar pulls the volume of the turbinate laterally, increasing the free space in the nose. Although all types of cautery lead to some loss of functional mucosa, they are popular, because they can be performed in an office setting, under local anaethesia, with minimal discomfort for the patient. Also, it can be repeated in the future, if so decided, although too many redo’s can lead to excessive scarring of the turbinate and impair the functional efficiency of the nasal mucosa. Postoperatively, some crusting over the turbinates is expected, for which clinic appointments for debridement will be needed.
Submucous Turbinoplasty: If the bony part of the turbinate is too large, the surgeon can remove part of it, along with its mucosal cover. The operation is done under general anaesthesia and endoscopic control.
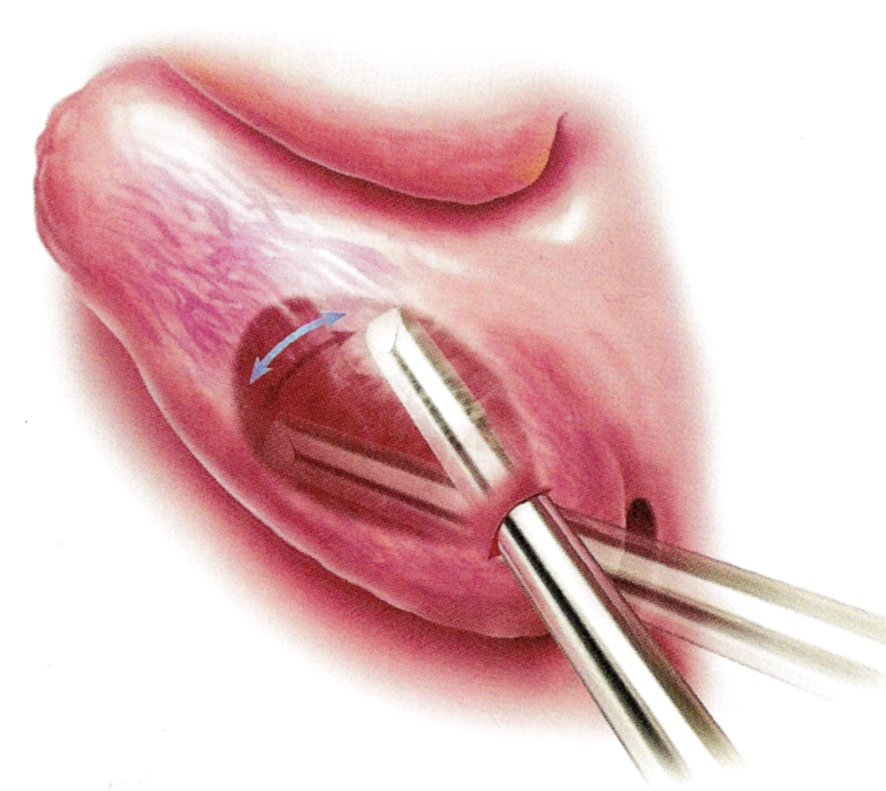
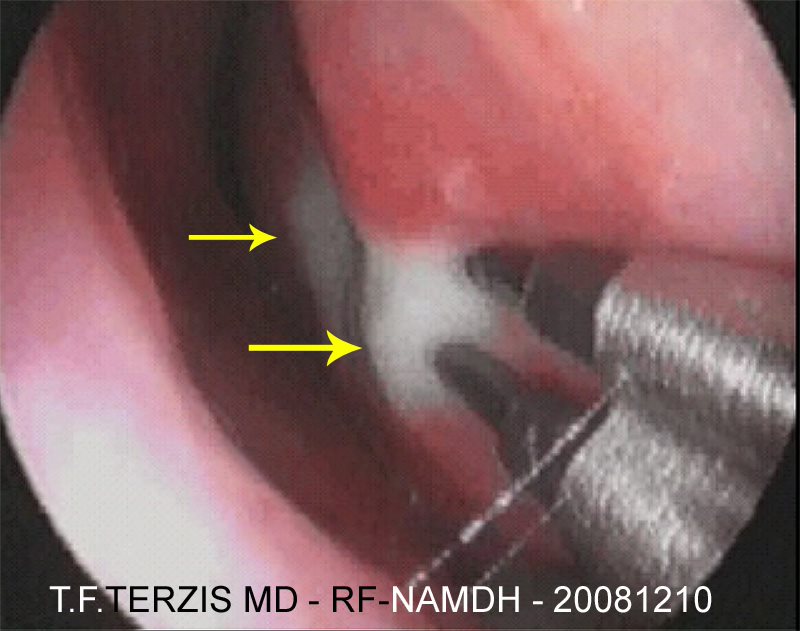
Partial Submucous Turbinectomy with the microdebrider (shaver): A small instrument, of 2 mm diameter, is inserted under the superficial lining of the turbinate, via a 2 mm incision (photo N007). The rotating blade at the tip cuts the excessive soft tissue and the suction removes it. The procedure requires a general anaesthetic and can be done either under endoscopic control or with conventional instrumentation. This is the method we prefer in our Unit for patients undergoing surgical straightening of the septum, as it creates less trauma and scarring, and has the least postoperative crusting.
This website aims at providing simplified scientific information and not medical advice on specific conditions or individual cases. In this respect, it cannot replace the consultation and documented opinion of a specialist physician.